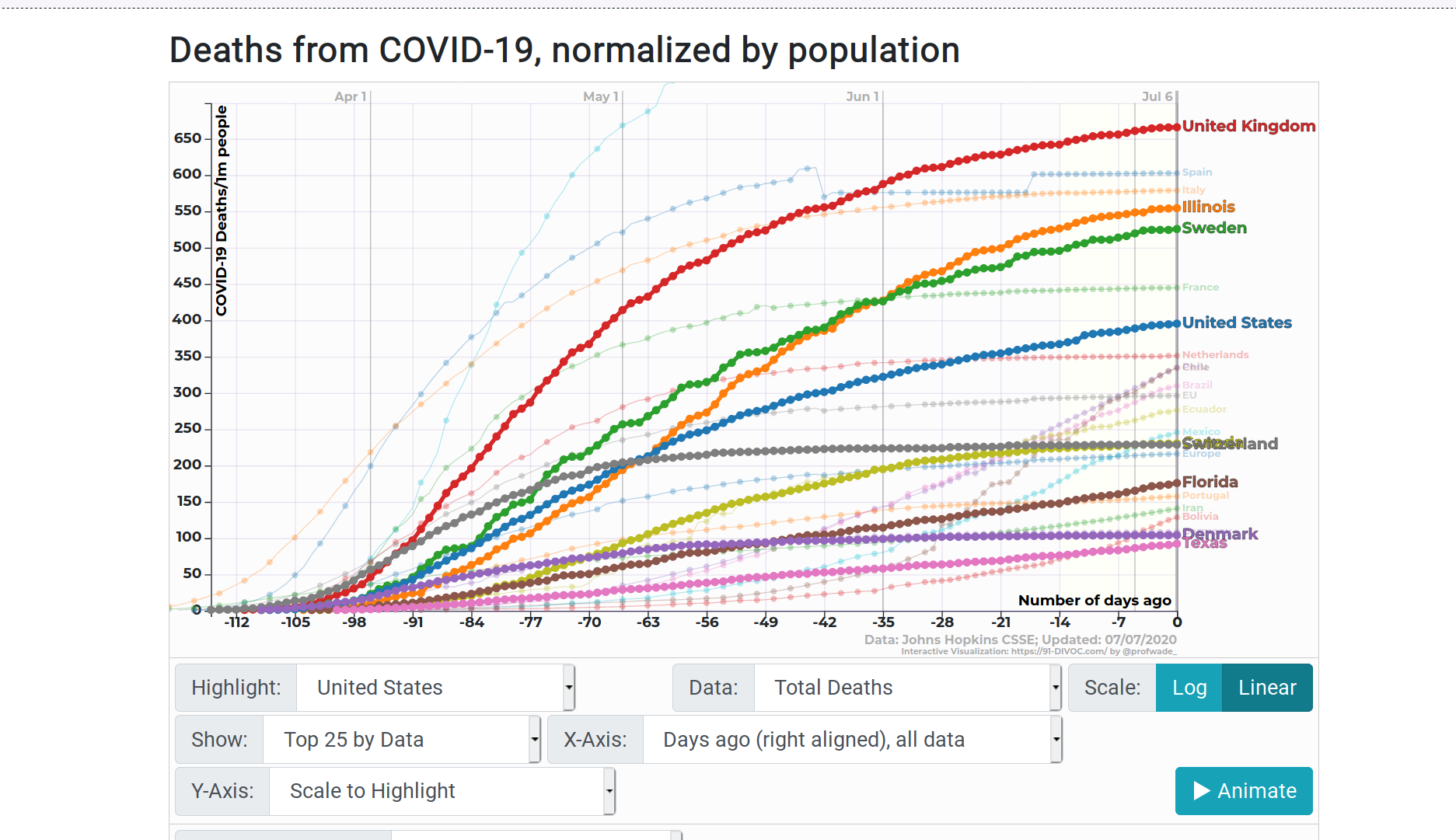
(The country you can’t see, overwritten by Switzerland, is Canada.) What I make of this is that maybe the Swedish approach, relatively unrestricted, works about as well as the Illinois approach, pretty locked down except for big demonstrations. Otoh, if the Danes are similar to Swedes, then the former nation’s lockdown might have been quite helpful in reducing deaths. To a level almost as low as Texas, tho we’ll see how that works out in the coming month or so.
Go play with the site, recently enhanced to allow comparisons between U S states and nations. It’s great fun.
It’s pretty well-known that medical care is absorbing an increasing proportion of GDP, and putting many Americans into financial (and, in many cases, medical) distress. One source of the problem is poverty– people whose incomes are too low to afford decent housing, food etc. are unlikely to have much left over to pay for medical treatments. And another cause might be an aging population who demand advanced treatments to further extend their lives. Both important issues, but this post focuses on another, probably more important one: The medical system is full of rentiers and other thieves, who, pretending to improve health or efficiency, impose tolls or promote unnecessary treatment, resulting in higher and rising costs. That’s the book Marty Makary (MD) has written.
Using a conversational style, well-organized, packed with personal anecdotes, Makary, a cancer surgeon at Johns Hopkins, works his way thru some of the reasons medical care costs so much. Sources are meticulously cited in endnotes. I think his findings can be pretty well summarized:
Some medical professionals offer screenings and other promotions to entice folks to get treatment they really don’t need.
Hospital charges are, not quite random, but pretty much void of any relationship to actual costs or what other customers pay for the same service.
Some hospitals take advantage of their quasi-monopoly status to charge excessive prices, and aggressively sue customers who don’t pay promptly. On the other hand, at least a few hospitals in similar circumstances find they can prosper while charging more reasonable prices.
Air ambulance (and, to some extent, surface ambulances) have been largely taken over by private equity firms, and impose excessive (mostly unregulated) charges on people who are in no position to bargain.
Some doctors are outliers in terms of types of birth delivery and various surgeries, meaning that they perform invasive and/or expensive procedures at a much higher rate than the norm. This may be because they’re selfish and inconsiderate, or maybe they just haven’t thought about it and, when shown the data, mend their ways.
The opioid problem, as reported elsewhere, is partly due to some doctors prescribing more pills than really necessary.
Overtreatment is a problem; often a more conservative approach is more effective (as well as less expensive).
A few organizations have managed to rethink how medical care is provided, giving more autonomy to practitioners as well as more support to patients. Also, a few payers (meaning, typically, employers who pay for insurance) are managing to learn the charges imposed by various providers, and incentivizing their insureds to choose less costly providers.
“Health insurance,” which is really a care financing arrangement and not insurance in the conventional sense, is an even sleazier business than I thought, and insurance brokers are incentivized to maximize costs.
Pharmacy benefit managers may have seemed like a good idea at one time, but basically are toll collectors between the payer and the drug provider. Similarly, “group purchasing organizations” charge a toll on hospital purchases of equipment and supplies. In both cases it’s rarely possible to get accurate data on who is paying who how much for what.
Then there’s the “wellness” industry. Of course sensible diets and some exercise are good things, but “wellness” seems to have evolved to divert attention from the main causes of escalating costs.
The book concludes with a few recommendations, mostly for providers and legislators, but also for consumers, who are encouraged shop around, and ask for prices before agreeing to treatment.
A few important concepts are missed.
The scandal of “Certificate of Need” laws, which protect hospital monopolies and still exist in several backward states, isn’t mentioned.
While the cost of drugs receives attention, no mention is made of the patent games by which the U S Government enables drug manufacturers to extend protection, and collect rents, far beyond the statutory period.
Little attention is given to the history of medical care in America, including lodge practice and the role of wealthy foundations in choosing how medicine developed.
Finally, I hope the next edition will avoid doubling the populations of Missouri and Wisconsin (page 79).
Reportedly, taxes of 163,036 parcels in Cook County were not paid on time. This comprises 2018 taxes which should have been paid in 2019. and amounts to 8.7% of all parcels in the County. For a dozen south Cook County municipalities, this amounts to 20% or more of total parcels. Counts by municipality are posted separately for south, west, and north Cook. All sources show the percentage of parcels with unpaid taxes within the City of Chicago as 9.9%.
Separately, the reports show that only 7.8% of the delinquent taxes offered for auction in 2018 were bought by investors, which might imply that the remaining parcels are considered worth less than the taxes owed.
Unfortunately the source doesn’t tell us how many of the parcels are vacant, residential, commercial, or other uses, and gives no historical context, so we don’t really know how any of these figures compare to prior years. But regardless, the current numbers are alarming.
Suppose that the real estate tax system was changed, so that improvements would be tax-free while the value of land as vacant would be heavily taxed to make up the difference. For vacant parcels, construction of houses or other structures would not increase the tax. For parcels which contain improvements, taxes likely would be lower than now, and improvements would again be tax free. Just a thought.
Maybe expanding tax-exempt institutions raise land prices?
Crains tells us that a strikingly-designed two flat, less than 30 years old, is worthless. Well, they didn’t say it quite that way, but it was sold for $1.9 million to a buyer who will demolish it. So the $1.9 million was for the land. I don’t know whether any developer of housing or anything else taxable would have paid nearly that much for the site, but the buyer was tax-exempt Illinois Masonic Medical Center. Their exempt status of course made the land more valuable to them. Which raises the interesting question of whether buying land in the path of such an institution’s expansion might be a profitable strategy. Of course, a fair-minded community might decide to tax land used for hospitals at the same rate as land used for housing and other useful things. But we’re not there yet.
“Taxes – De Standaard” by Stijn Felix is licensed under CC BY-NC-ND 4.0
Over at New City, Tony Fitzpatrick tells us how he survived a heart attack. The good news, of course, is that he did, and it seems to have been due to an aware spouse, responsive ambulance, and nearby hospital with skilled and dedicated staff. Except for the first, those are advantages of living in a more-or-less functional and prosperous city, with pretty decent emergency services, all of which is reflected in the cost of land.
But somehow, because before “ObamaCare” Tony’s pre-existing condition prevented him from getting insurance for medical expenses, he credits O’Care with his survival. As if, five years ago, there were no ambulances, no hospitals, or no medical staff. In 2010 an ambulance still would have come, he still would have been taken to the closest available hospital, and the staff still would have done their best for him. The only difference is that, afterwards, he would have gotten a big bill, even bigger than the bill he probably did (or will) get. He might have paid the bill, or worked out some payment plan, or had to sign up for some kind of public assistance. And very possibly the hospital would have written off part of the bill. (Either way, before or after O’Care, the hospital would have a considerable staff who spent their time negotiating payments, filling out forms, etc.)
It wasn’t Obamacare, Tony. It was living in a city with helpful people and pretty good medical services. Either way, we’re all paying for it.
And, yeah, somebody ought to make this comment on Tony’s article, but I can’t seem to get thru New City’s spam protection. Maybe someone else can.
I am not going to call it “Obamacare” since most of it existed long before we’d heard of that guy, and I am not going to call it “health insurance” since it only applies to medical costs, which have just an approximate relationship to health, and it is not insurance since it is intended to pay routine costs rather than help pay for catastrophes. I suppose I might call it “diversion of productive people’s income to lobbyists and their clients” (which we might pronounce “DOPPILC”), but I’ll just call it “govcare” since it certainly involves the government and has something to do with care.
I really don’t understand it at all. Do we, the People of the United States, wish to pay whatever is necessary in order that all of us may have whatever medical treatment a group of licensed professionals assert is necessary? If so, why do we think it will not absorb 100% of our production beyond subsistence? If not, how do we decide priorities and set limits, when inevitably any limit is going to find someone very sick and very sympathy-arousing unable to afford some treatment which really would be helpful? (The answer probably has something to do with us the People of the United States behaving like adults, but if I was the very sick person in question I might have a different attitude.)
The subject is simply too big for me to comprehend, so I will just nibble around the edges. Today’s nibble is a message I received from the “health insurance” company who take a large part of my income.
Copayments do not apply to deductible or out of pocket.
Or, to put it a different way, if you purchase any considerable amount of medical treatment, what comes out of your pocket is likely to exceed the “out of pocket limit” that “your” “insurance” company proclaims. (This is in addition, of course, to the amount they already took from you to provide what they call “coverage.”
From C. Eugene Steuerle’s June 27, 2012 statement at http://www.urban.org/UploadedPDF/901508-Marginal-Tax-Rates-Work-and-the-Nations-Real-Tax-System.pdf
I’ve written before about the wild effects of graduated taxes and means-tested benefits which can dump low-income workers into effective tax brackets in excess of 100%. That is, once the effects on eligibility for earned income tax credit, child tax credit, medicaid, SNAP (food stamps), subsidized housing, and so forth are taken into account, an extra $1000 of income can easily cost more than that amount in increased taxes plus reduced benefits. (Worse, most low-income people don’t have professional accountants who keep track of this, and so they don’t know in advance what the effects of getting a raise, or taking some overtime, might be.)
This is hardly original with me, and most recently the Congressional Budget Office has issued a report on the subject, summarized here by Evan Soltas of Bloomberg. What can be done to fix this? Not much, conclude most writers including Soltas. We need tax revenue, we need to target aid to those with the greatest need, we can’t expect the rich to pay everything (since they have the lobbyists, lawyers and accountants to limit the taxes they pay.)
None of the writers who get attention seem to consider the citizens dividend. The basic idea is that government collects all the land rent — that is, the effective rental value of private control of natural resources — and share it with all citizens, everyone getting an equal share. It’s done on a small scale in several jurisdictions, including Alaska where each state resident gets a thousand dollars or so, each year, as a share of investments funded by mineral resources. Of course, natural resources include not only oil, gas, and ore, but also the electromagnetic spectrum, agricultural land, forests, and much of the value of land sites (except of course those which have no market value.) Suppose this rental value, or just a substantial part of it, were collected by the federal government and distributed, equally, to every U S citizen (maybe legal permanent residents should get a share also). How much would that be? Would it be enough to pretty much replace most means-tested programs? Wouldn’t that solve our problem?
Of course, arguments for collecting economic rent go far beyond fixing the screwed-up incentives of means-tested programs and graduated income taxes, (visit a Henry George School or the Henry George Institute to learn more), but let’s not forget this benefit.
And by the way, it isn’t only the poor who can face these >100% marginal rates. I wrote before about how certain Cook County homeowners with incomes in the $75,000 – $100,000 could face such rates; I don’t know whether these limits remain in effect. More broadly, it seems that affluent Americans subject to Medicare face a similar situation: As explained here, should your “modified adjusted gross income” amount to $107,001, then your Medicare cost will be $754.80 more than if your income had been only $107,000. The effective tax rate on that particular dollar is 75,480%. (Of course if you have a really alert accountant keeping track of all your financial affairs, she will alert you and find a way to avoid that extra dollar. And that accountant knows that the rates quoted above are for 2011 income, at least I think they are, and different limits will be in effect for the current year.)
Last month a couple of my dependents went to the local hospital for routine blood tests. The hospital sent me a routine bill for an outrageous amount, saying “don’t worry about this, we have asked your insurance company to pay, and you are responsible only for the portion they don’t pay.”
A few weeks later, the “insurance” company, popularly known as “Blue Thieves,” sent me a statement, and the hospital sent a revised bill. These show that the insurance company paid exactly zero, but muscled the hospital’s fee down by 75%. Both parties expect me to pay the difference. In other words, if you are a normal retail customer, the hospital marks up your bill 300%. In my previous experience, lab costs are typically marked up this much or more; for other services the markup is often less.
To reduce your medical costs, then, just tell the hospital that you’ll pay what Blue Thieves pay, 25% of retail.
I put “insurance” in quotes because what they sell is mainly not insurance, in the sense of taking on some of your risk, but protection, in the sense of “we will impose extra difficulties on you if you do not pay us.”
Yes, the report of the Financial Crisis Inquiry Commission is out. It’s over 600 pages long. Sources I respect say it’s the expected whitewash. I probably won’t ever read it. I still haven’t read the Obamacare Act (yeah, thats not a good name for it, we really oughta call it something like DemoPublicare.) Anyhow, I just found out how it’s going to increase the screwing up of the housing market.
a highly targeted 3.8% tax enacted as part of the controversial health-care reform legislation that has been signed into law and which Republicans are now trying to overturn.
The tax will apply to individuals with adjusted gross incomes above $200,000 and couples filing jointly with more than a $250,000 AGI. If you and your spouse choose to file jointly, the AGI threshold is $125,000 for each of you.
The Medicare tax, so named because the proceeds are to be dedicated to the Medicare Trust Fund, will be on interest dividends, rents less expenses, and capital gains less capital losses. But the key thing to remember is that the tax is based on whichever is less, the gain you made on the sale of the house or the amount your income exceeds the AGI threshold.
It’s complicated, so it’s hard to predict how it will effect every seller. As always with tax matters, it’s best to consult with a professional.
Of course, the income limits may change (legislatively or thru unmeasured inflation), so any of us who own our housing better save all receipts which might possibly have anything to do with adjusting the basis. But at least it doesn’t immediately affect the rest of us, does it?
Not so. I’d say this is another in a series of moves discouraging old people from selling houses that are larger than they need or really want, and which would otherwise be bought by families with children who could use the space. Earlier policies with similar effect include real estate tax breaks targeted at old people, and whatever programs facilitate reverse mortgages.
So what will homeseeking families do? Most likely, they’ll find houses they can afford, and the probability is that these will be further out. (The tax presumably also applies to sales of high-priced vacant lots, another force discouraging construction of homes on well-located sites.)
So maybe instead of the Obamacare Act, we should call it the Sprawl Enhancement and Old People Stabilitzation Act.
 It’s pretty well-known that medical care is absorbing
It’s pretty well-known that medical care is absorbing